
Re: Walmart Health: Just had a great dental visit this morning, which was preceded by helpful reminders from Epic, and…
Monday Morning Update 1/5/09
NYC offers $60 million in subsidies for eClinicalworks EMR, with doctors in the poorest neighborhoods receiving the most assistance. One doctor notes how their program may vary from other initiatives around the country: “We know that at these fancy schmancy systems, they can do these things, but here in New York, we’re trying to do this for the storefront in Harlem.”
In another not so “fancy schmancy” part of the world, the Maine Health Access Foundation announces new low-interest loans to promote EMR adoption in primary care medical practices.
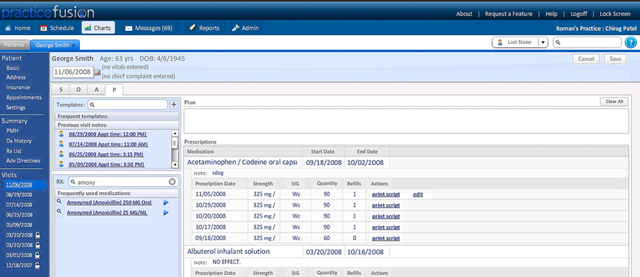
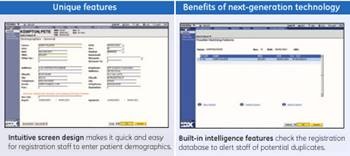
"Free EMR" vendor PracticeFusion has always been questionable to us because their announcements seem to invite more "confusion" than "fusion" (i.e. misleading claims of a Google partnership, announcements of rapid growth that didn’t seem all that rapid, the company’s business model of selling de-identified patient data and pushing ads, how to get the records back out if the honeymoon sours) but the company seems to be playing seriously, bringing on management talent and releasing a good-looking 2.0 product (click above to enlarge). I’m starting to feel more convinced, although it’s hard to know how deeply doctors are actually "using" the product instead of just signing up for it because it’s free. That’s true of all vendors, though — the real question is what functions are being used, by whom, and with what result? We’ve yet to run across a real, live PracticeFusion user, so if you know one, let us know. Surely if it’s anything but terrible someone must be using it — it’s free and online.
Housekeeping reminders: put your e-mail address in the Get Instant Updates box to your upper right to hear first about new HIStalkPractice news (you need to sign up here even if you get HIStalk updates since they are separate). Click the Email This to a Friend graphic to tell you pals about HIStalkPractice (pretty please!) You can search across all HIStalk sites with the Search HIStalk Sites Google box, also to your right. Lastly, we need participation: readers, commenters, guest article writers, interview subjects, and rumor reports, so e-mail us anything helpful.
The New York Times overviews the Marshfield Clinic’s (WI) use of technology and an EMR. The article discusses the potential EMRs have for improving healthcare, especially as patient data is mined to find patterns (e.g. outcomes) to manage chronic diseases. Marshfield leaders emphasize that measurable ROI is not the key to assessing the EMR’s success. I wonder if the Harlem and Mainer docs agree.
Outgoing HHS Secretary Mike Leavitt’s editorial in the Washington Post that we mentioned last week urges that any government "investments" in healthcare IT be limited to systems that are CCHIT-certified as interoperable. One might argue that the government should not be intervening in the EMR market by trying to pressure vendors to make them interoperable (a theoretical capability) than to pressure providers to actually share information in whatever way the government has in mind and then let them pressure vendors themselves. Just because you own an "interoperable" EMR doesn’t mean that you’ll ever actually exchange data, either because you as a practitioner don’t want to or because there’s no organization technically prepared to accept your information in the first place.
The local paper highlights Tucson physicians who are moving to EMRs. A former EMR resister believes the transition is “hands-down better for the patent because there are much fewer things you miss." He also notes that his productivity dropped from 25 to 10 patients a day during the changeover to NextGen, but has presumably improved since. The administrator admits the ROI is not immediate, though there is immediate improvement in patient quality care.
Forbes quotes a Congressional Budget Office study that says EMRs will save $7 billion over five years. So given the thousands of EMR-using practices out there, doesn’t that constitute a pilot study group that should already be saving those dollars? The problem, of course, is that it isn’t the practices that are saving the money, most likely, so poring over their books would probably show nothing but additional EMR expense since the savings accrue to insurance companies, patients, and employers. The article cites several self-proclaimed experts, none of whom appear to actually practice medicine and, in fact, all of whom make money selling EMRs and related services. The reporters who write these articles always seem to marginalize the concerns and observations of real, practicing doctors, writing them off as irrelevant Luddites when there are fast-talking sales types available who, not surprisingly, sing the praises of whatever they’re selling at the moment.
GE Healthcare releases Centricity Business 4.3. I assume Centricity “Business” is the old IDX software since it is geared to academic medical centers and large practices.
Sermo introduces a new infectious disease monitoring tool called Sermo FluMonitor that allows physicians to report geographically based clinical observations in real time. I’d love to see how the reliability compares to Google’s flu trend tool.
A new report notes the shift from a provider-owned medical record to a record shared and controlled by both the provider and patient. It predicts the EMR market will grow by 14.1% annually through 2012. Of course I remember the days when everyone predicted 30% per year growth, a rate the market never quite achieved.
A UMass study says that medication errors occur in 7% of adult chemotherapy visits and 19% of those of children. The biggest question that lay people and even clinicians often forget to ask is whether the "errors" actually had the potential to cause patient harm without being caught down the line. The authors of this study did ask and found that about half had that potential, with most of them involving failed reconciliation between initial chemo orders and those adjusted for a specific visit. Many of the errors were cause by people in the home preparing and giving doses, not medical professionals. The clinic with the lowest rate of errors, one per 500 visits, used an EMR system with physician order entry.
Financial conditions are hitting physicians: more of them want hospitals to pay them for on-call cover or to hire them outright and fewer of them will attend conferences that involve overnight travel in 2009. Another example: a practice management company for plastic surgeons is laying employees off this week, which might logically be interpreted as meaning that fewer people are willing or able to shell out for cosmetic surgery.
Here’s a significant but tiny news item that the usual healthcare media will probably miss (unless they read it here, of course). A primary care office in Maryland cancels its plan to move to a boutique practice model when the Maryland Insurance Administration, worried about losing more primary care doctors, held hearings to decide whether retainer-based medicine is a form of health insurance that requires additional state regulation. Is it insurance to charge patients a flat yearly fee rather than fee-for-service? My first reaction was an emphatic no, but I can see how there is some gray area that would need to be carefully spelled out in whatever agreement the patient and practice sign. Other than that, it’s still an emphatic no in my book, but I’m not a state insurance bureaucrat. My suspicion is that the state wouldn’t have cared if it was a small group doing it.
Medical bills that have been turned over to a collection agency are keeping many people from qualifying for a mortgage, a mortgage company says, calling it a "huge injustice" that credit scores are hurt even when the debt is fully paid. I’ll go out on a limb to speculate that those mortgage companies who can’t get the money owned to them without turning it over to a collection agency (or who even experience only ‘slow pay’ from debtors) feel it’s entirely right and good that their deadbeats take a credit score hit.
I’ve always found the Zagat restaurant surveys to be pretty reliable. As Zagat expands into healthcare, we’ll see if the results will be as solid. The new Zagat Health Survey tool, offered in partnership with BCBS North Carolina, allows patients to evaluate their physicians on a set of distinct criteria. I wonder if consumers are as willing to rate their doctors as they are a good meal.

This is Inga’s kind of doctor. An Irvine plastic surgeon sets his Botox rates based on the rise and fall of the Dow Jones industrial average ($1/Botox unit for every 1,000 points on the Dow.) On those days his patients open their 401K statements and become depressed by all those losses, they can now find consolation from a little cosmetic refresh.
I believe California already has laws on its books like Maryland is contemplating – the Knox/Keene Act, iirc. I don’t encourage legislation myself, as a rule, but the position could be a valid one: what kind of consumer protection needs to be in place for those who might entrust all of their medical care to a single source?
This month marks my 1 year anniversary for using Practice Fusion for my half-time private practice as the exclusive method of charting. I use it every day and i operate a 90% paperless practice. I am a technophile but even more than that i am a productivity-phile. Over the last 10 years I’ve used a half dozen Emrs and tried another half dozen. For my purposes, Practice Fusion is one of the best for speed and ease of use, including features that i need, and for cost. Sure they are new and dont yet have all the bells and whistles of the more established products & vendors, but this is changing fast. They are also eager for feedback from doctors to continually make their product better. What i think will drive their survival and growth in the marketplace is that they will live and die by making their product appealing to physicians since their subscriber base will drive their ad revenues. In addition, if Practice Fusion becomes a viable player (I think they already are) what physician will continue to spend $5k to $40k for an EMR that they could get for free? The ads are unintrusive and the majority are not pharmaceutical ads. I’ve seen ads for vacations, new cars, even naturopathic treatments. The post above mentions “selling de-identified patient data” –everyone should be aware that ANY EMR vendor can do this without the physician or patient’s permission–it is provisioned within the infamous HIPAA policies. Therefore, why not let those revenues help my bottom line?