
News 1/13/09
From Dr. Old-timer: “Re: Obama’s EMR plans. Do you think that Obama read the National Research Council Report before he suggested that all medical practices are computerized within the next five years? Does he understand that no one is quite sure the overall effect on quality and costs? If I understand the basics of the report correctly, it sounds like we lack adequate functionality in our existing products. So we need better products, need money to build those products, need money in the hands of providers to buy those products … all in the next five years. It will never happen.” Clearly we need to see a roadmap that details how Obama and team plan to get there and how to pay for it. But, I have to agree that five years is a tight timeline. First, I have my doubts that Congress can act quickly. In these post-bank and automotive bailout times, I don’t see anyone agreeing to pass out money without a plan that includes specific goals and plenty of oversight. And don’t forget the privacy folks will want to issue their stamp of approval. If and when Congress passes a plan, who is going to administer the money and to whom? Will vendors need to rewrite software to meet new governmental requirements? It’s all a big mountain to climb.
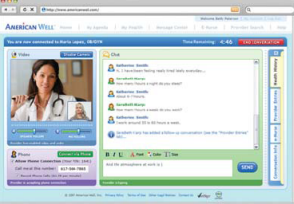
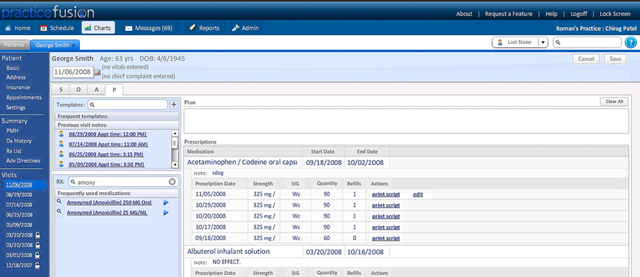
From Early Adopter: “Re: Practice Fusion. While I am glad Dr. Thakkar found an EMR that works for him, I would never take a similar risk. About 10 years ago I found a slick EMR product developed by a local start-up and got a great deal for being one of their first clients. They, too, were ‘eager’ for my feedback and making the product better. However, two years after going through all the pains of implementation, the company went bust. My current vendor converted all they could, but there are definite gaps. Sure, I like the idea of a free EMR and I don’t mind the ads. I even like ease of use and speed. But I will never again go through the hassle of implementing any software if I am not confident in the vendor’s business model and long term viability.” If you missed Dr. Thakkar’s positive comments on PracticeFusion, you can read them here.
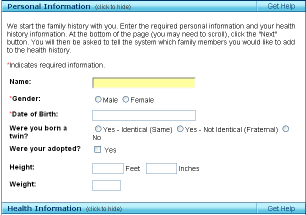
The acting Surgeon General announces the release of a new version of "My Family Health Portrait," yet another personal health record, but this one’s from the government. I think they goofed in putting the password to the Tuesday media conference in the press release for the whole world to see, although I don’t expect too many eavesdroppers to jump on. Given the number of misspellings and grammar errors on the site itself, maybe that’s not surprising.
Two US Senators introduce the Health Information Technology Act of 2009, which they hope will serve as a blueprint for addressing health care issues in the upcoming economic recovery package. The HIT Act would establish grant money for health care providers to purchase (or lease) HIT systems. The grants would target safety-net and rural providers. Maybe it will be more successful than the HIT Acts of 2005, 2006, 2007, and 2008. None of those bills ever passed.
Solo practitioners are being especially hard hit by economic conditions, according to an LA Times report that profiles the failed practice of a primary care practitioner in Beverly Hills. She hasn’t been able to pay herself for almost a year, spent $40,000 of personal savings and $15,000 in credit card debt to keep the practice going, and finally closed the practice to work for a Johns Hopkins-affiliated practice. She said patients stopped coming when the economy went sour and those who did often stiffed her on their co-pays.
Kentucky’s lieutenant governor, who is a physician, says the state will announce a collaboration of three state universities that plans to study whether healthcare IT is a good investment. While some of the state’s interest may be because Kentucky’s incidence of heart disease, obesity, and diabetes is among the top few states, the LG admits that the main plan is to get a piece of the billions the Obama administration may spend on healthcare technology.
Texas Health Resources Organization for Physicians (THRP) and MedSynergies Inc. create a new management services organization called Texas Health MedSynergies (THM) to offer physicians revenue management cycle services and other business functions. Texas Health’s goal is to “enhance engagement between physicians and our hospitals” and give providers more time for patient care. The pricing structure was not disclosed. Will the pricing be attractive enough to make it worthwhile for a physician to consider, or will the doctors prefer to keep their money matters as removed as possible from the hospital?
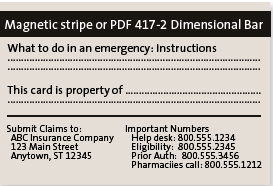
MGMA announces its Project SwipeIT initiative, aimed at advancing the adoption of standardized patient health insurance ID cards with machine-readable information. MGMA claims the industry wastes as much as $1 billion annually as a result of non-standardized cards. If every retail establishment can read every credit card in our wallet, and every ATM in the world can read our debit cards, how hard could it be to standardize an insurance ID card? As I patient, I roll my eyes every time a doctor’s office has to photocopy it.
Concierge Medicine of Las Vegas chooses PracticeOne.
In addition to shortages in primary care physicians, look for a shortfall of over 1,000 gastroenterologists by 2020. As the demand for colorectal cancer screening grows, so does the demand for gastroenterologists. The shortage could limit the nation’s ability to implement national guidelines for cancer screening.

The 33-physician Michigan Cardiovascular Institute (WI) selects Sage Intergy PM and EHR.

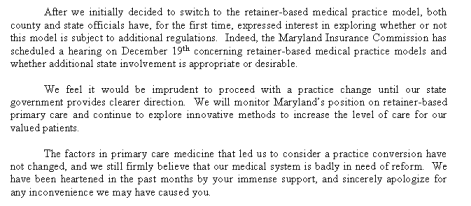
Long-time Misys Vision client Physician Associates LLC (FL) selects the Allscripts Enterprise EHR solution for its 80-physician practice. The CIO of Physicians Associates calls the decision a “no-brainer” since they liked their Vision product and the Allscripts EHR. (Don’t you know that made Glen smile?) Allscripts also announces that Tully-Wihr Company, in conjunction with Ray Morgan Company, signed an agreement to resell the Allscripts MyWay EHR/PM to 100 physicians. In addition, Excela Health (PA) contracts with Allscripts for its 115 employed physicians. MDRX stock (blue) is looking good against the Nasdaq (red) in the six-month stock price chart above.
MD-IT, a provider of medical documentation services and software for physician offices, closes on $11 million Series B funding from PE firm J. Burke Capital Partners, LLC.
An article in the current Annals of Family Medicine questions whether consumer drug advertising really works. Patients asked doctors about a specific new drug in only 3.5% of visits, far less than the 15.8% found in a similar study five years ago. The researcher isn’t sure if it’s because patients no longer trust drug companies or whether poor and non-English speaking patients decline because of drug cost and lack of advertising exposure, respectively.
A Texas woman sues her doctor for telling her she can’t get a handicapped parking sticker just because her arms and legs go to sleep, the rudeness of which, she claims, caused her to have a heart attack right in his office. A week earlier, she had sued her attorney for being sarcastic with her and the month before, she sued President Bush because mismanagement of the local housing authority may cause her to lose her home. The kicker is her recommendation to the doctor: he should get psychiatric help.
As we start our second full week of HIStalkPractice, we want to thank all you early adopters, especially those taking the time to provide us great feedback. This week, we will roll out our first guest writer, Dr. Joel Diamond, a part-time practice family physician and an experienced EMR user. He also serves as CMIO for healthcare interoperability company dbMotion. We think he is smart and funny and we know you will, too. We are also lining up an EMR implementation guru to provide great advice and commentary on maximizing the use of EMR. In addition, look for upcoming HIT Moments that highlight assorted other physicians and industry gurus. Make sure you have signed up to receive your HIStalkPractice updates – and hang on for the ride!















The article about Pediatric Associates in CA has a nugget with a potentially outsized impact: the implication that VFC vaccines…